Answer
THESE TWO PATIENTS COME TO YOU WITH FACIAL PARALYSIS.
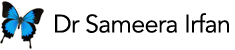
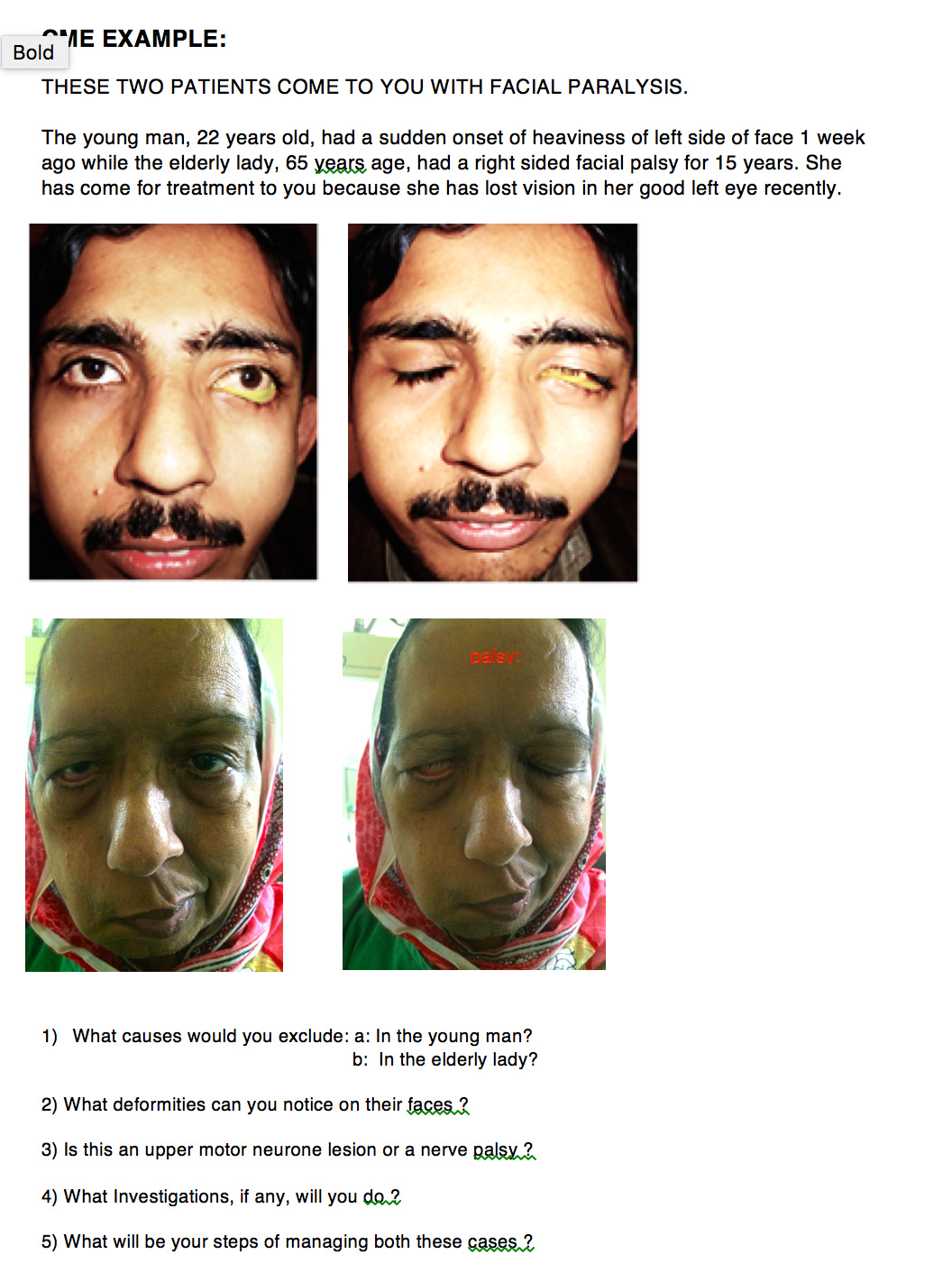
The young man, 22 years old, had a sudden onset of heaviness of left side of face 1 week ago while the elderly lady, 65 years age, had a right sided facial palsy for 15 years. She has come for treatment to you because she has lost vision in her good left eye recently.
- What causes would you exclude: a: In the young man?
b: In the elderly lady?
When you think of a cause of muscle paralysis, VISUALISE ORIGIN & THEN COURSE OF THE SUPPLYING NERVE.
Ans: When you think of a cause of muscle paralysis, VISUALISE ORIGIN & THE COURSE OF THE SUPPLYING NERVE.
Facial Nerve originates in the Brainstem (Pic 1) next to 6the Nerve Nucleus. So in a lesion involving the brainstem, it may also be affected; therefore in a NUCLEAR OR A LOWER MOTOR NEURON LESION, look for an abduction deficit in an eye (opposite eye as the 6th nerve crosses to the other side).
The facial nucleus (a lower motor neuron) receives commands from the Cerebral Motor Cortex (the upper motor neurons)> These cortico-nuclear fibres supplying neutrons, intended for upper facial muscles, come from both cerebral motor cortices to both facial nuclei. Therefor, in a unilateral brain lesion, the upper half of face is spared.
Facial Nerve emerges between pons and medulla on anterior surface of brainstem, then travels along the lateral wall of posterior cranial fossa along with the 8the Nerve to enter the Internal Acoustic meatus and then the Facial canal in petrous part of temporal bone.
So a tumour in this part of the brain will affect the Facial as well as the 8th Nerve.
When it is in the facial canal and passing through Internal and middle ear, it can get affected by lesions of these structures.
Finally, it exits the skull through the stylomastoid foramen. Here it lies close to the Carotid Artery. The nerve then runs forwards in the Parotid fascia and divides into its branches to supply each muscle of facial expression. (Pic 2)
Few of you have enumerated the causes and they are OK.
But your clinical examination should give you a clues as to what exactly is the site of Nerve Palsy. And that should decide your investigations.
2) What deformities can you notice on their faces ?
This young man had an acute problem. The left brow fold is very much there.
There is no flattening of the forehead or drooping of the brow.
His LOWER PART OF FACE IS AFFECTED, UPPER PART IS SPARED.
The upper lid normally comes down and covers the eyeball. Only the lower lid is affected with an ectropion, pooling of tears, lowering of the lateral cantonal angle.
Slight flattening of the nasolabial fold.
There is no Drooping of the angle of the mouth.
No Flattening of the cheek.
So IT IS A NUCLEAR INVOLVEMENT. THE FACIAL NUCLEUS RECIEVES INPUT FROM MOTOR CEREBRAL CORTEX OF BOTH SIDES OF BRAIN FOR THE UPPER PART OF FACE.
AN MRI IS MANDATORY TO FIND THE EXACT SITE OF BRAIN LESION: TUMOUR, DEMYELINATION.
This lady has a long standing typical Facial
Palsy. All facial muscles are hanging downwards due to the affect of gravity:
Forehead is flattened. Upper brow is drooping, upper and lower lids are sagging downwards, as well as the lateral cantonal angle.
Flattened cheek, nasolabial fold, drooping of angle of the mouth and chin, deviated mouth. Inability to close the lids resulting in corneal exposure.
So long standing cases, no need for any investigation. Rule out Trauma, Brain Surgery, Diabetes, Hypertension, any health problem only by history.
3) Is this an upper motor neurone lesion or a nerve palsy ?
By proper examination, you get the site of involvement.
i) In an expected Nuclear Lesion, must always check taste on anterior half of tongue . WHY ????
ii) WHY NO TASTE ABNORMALITY IN A SUPRANUCLEAR LESION INVOLVING THE CEREBRAL CORTEX ???
iii) IS FACIAL NERVE PURELY A MOTOR NERVE /
iv) HOW DOES IT CAUSE A DRY EYE???? BY WHAT MECHANISMS????
These questions we will discuss in the tutorial!
4) What Investigations, if any, will you do ?
Depends upon the cause and site of involvement.
5) What will be your steps of managing both these cases ?
- The young man is an emergency: needs an urgent MRI Brain and a neurosurgical referral. Do not waste time looking for a neurosurgeon, get an appointment for an MRI first.
- In the meantime: protect the eye ball from drying up::
a: by lifting up the lateral lid margin with a surgical tape.
b: Lubricants: drops during day and ointment at night.
c: taping the lids together at night.
iii) Active physiotherapy to the involved muscles: tell him to close his eyelids forcible, blow balloons, purse his lips and clench his teeth.
These steps should continue even after his neurosurgery till full recovery occurs.
The Lady: all her facial deformities could have been prevented by above mentioned measures.
Now she needs extensive plastic surgery, which I did.
Step 1: Brow lift and taping upwards the lateral cantonal angle: Pic 3
Step 2: Lifting lower lid, medially and laterally, lifting of cheek and angle of mouth, at the same sitting via micro-incisions , under a local anesthesia. Pic 4