 27 May 2013
27 May 2013
Concept of A LACRIMAL FUNCTIONAL UNIT (LFU)
It comprises of the lacrimal gland, Ocular Surface and a Neural Network to provide a feedback from ocular surface to the lacrimal gland. Only that amount of tears are produced as are required by the ocular surface, depending upon the information sent to the lacrimal gland through the neural network.
Pathogenesis of dry eye: A multifactorial disease. Either it results from reduced tear production with increased tear osmolarity & an inflamed ocular surface. Or increased tear evaporation due to deficiency of lipid layer. Or poor wetting of ocular surface causing dry, damaged corneal epithelium. Even in presence of adequate tear production.
Lipid layer deficiency: due to meibomian gland dysfunction → Tear evaporation.
Aqueous layer deficiency: in KCS which is divided into: SS (Sjogren’s Syndrome) as in RA, SLE, Multiple sclerosis and Non-SS KCS: in pregnancy, postmenopausal women, HRT
Mucin deficiency: Stevens Johnson syndrome, chemical burn, Trachoma, Ocular cicatricialPemphigoid → Poor Wetting of Ocular Surface.
Predisposing Factors for Dry eye:
Old age: usually seen in post-menopausal women.
Connective tissue disorders
LASIK : lifting of corneal flap damages corneal nerves.
Drugs: beta blockers. antihistamines, AGT.
Diabetes: Type 2, impaired autonomic innervation to lacrimal gland, reduced corneal sensitivity, poor lac. Gland microvasculature, advanced glycation products activated cytokines.
Vitamin A deficiency
Effects of Ageing:
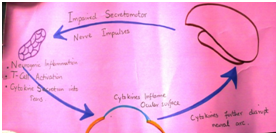
Ageing causes androgen deficiency. Estrogen & androgen receptors are present in the lacrimal & meibomian glands. Androgens are trophic for lacrimal & meibomian glands. They are potent anti-inflammatoryagents ( TGF beta) & suppress lymphocytic infiltration of lacimal glands. Androgen def. causes inflamed lacrimal and meibomian glands, with tear def. & hyperosmolar tears. These cause a pro-inflammatory environment on ocular surface. Also cytokine production and T-cell activation further inflame ocular surface, disrupt the neural arc.
Cytokines inhibit neuronal function. They convert androgens to estrogens and increase the level of tissue degrading enzymes
MANAGEMENT OF DRY EYE
It is a STEP-WISE APPROACH. It is important to listen to patient’s symptoms, find and eliminate the predisposing factors and find and treat the cause. Simply prescribing artificial tears does not work. This is an ocular surface disease; unless a wetting surface is restored, loading the eye with tear drops is useless.
Smptoms: Burning, Blurring of vision,Photophobia,paradoxical tearing.All symptoms are worsened by smoking, reading, computer work. Find the predisposing factors by a careful history.
Examination: aim is to find the cause resulting in a dry eye and to grade its severity. Grading decides the step-wise management and helps in assessing improvment on follow-up.
Grading of Dry Eye: according to symptoms & signs
MANAGEMENT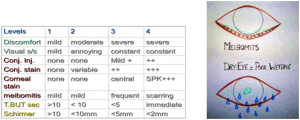
LEVEL 1: LEVEL 2:
1: Environmental & dietary modification Pt. symptoms don’t improve, T BUT &Schirmer =/< 10
2: Eliminate the cause. Add: Anti-inflammatory therapy:
3: Artificial tears. steroids, CsA, omega 3 fatty acids, Tetracyclines
4: Eyelid therapy. Punctal plugs
Tetracyclines: antibacterial, anti-inflammatory, antiangiogenic, reduce lipase production→ FFA→stabilize tear film.
CyclosporinA : increases aqueous &meibomian sec., increases goblet cell count, decreases cytokines & inflammatory cells in conj.
LEVEL 3: LEVEL 4:
If symptoms are severe, conj. & central corneal staining; Severe symptoms, SPK+++, conj
TBUT & Schirmer< 5mm Scarring/symblepharon, TBUT
Permanent punctal occlusion immediate, schirmer<2mm :
Autologous serum Systemic immunosuppressant drugs.
Soft contact lens Surgery: amniotic or mucus membrane graft, lid surgery, tarsorrhaphy
Autologous Serum: Contains trophic factors which promotes growth & migration of epi. cells. immunoglobulins, vitamins & are non-antigenic. Containdications; HIV, Hepatitis B, anaemia. Complications: bacterial keratitis, conjunctivitis, scleral vasculitis & melting.
FOLLOW-UP
1) Note subjective improvement.
2) Check the status of lid margins, cornea, tear meniscus.
3) Perform Schirmer’s test & TFBUT every visit to gauge efficacy of therapy.
4) NOTE: 3 layers of tear film; 3 tests to diagnose the abnormality of tear film.